Prostate cancer is the most common cancer diagnosed among men in America. For patients experiencing common symptoms, their provider will most likely order further testing to determine whether they are indicative of cancer or another disease. There are a number of methods used to test for prostate cancer, usually beginning with a physical examination and PSA testing.
Diagnosis
For many decades, prostate cancer has been most commonly diagnosed with a blood test called the Prostate-Specific Antigen (PSA) test, which measures the presence and levels in the blood of a specific protein produced by the prostate. PSA tests have been able to detect many prostate cancers which would not have been detected otherwise.
Typically, men with prostate cancer register higher levels of PSA, but high levels are not necessarily indicative of cancer; they may also be related to infection, enlargement, or inflammation of the prostate. Since the PSA test is only a screening test, when a man’s PSA is elevated, a prostate biopsy is often recommended to specifically diagnose prostate cancer.
The Jackson Clinic also currently offers prostate cancer biomarker testing with the 4 K Score®. If you are interested in having this test performed, please contact our urology department to make an appointment.
A newer technique, called MRI (Magnetic Resonance Imaging) Fusion Biopsy, involves an MRI performed prior to the biopsy and is more accurate than ultrasound at detecting prostate lesions.
Click the image below to view and download an informational PDF about this procedure.
A traditional biopsy, also called a transrectal biopsy, is usually performed in conjunction with a transrectal ultrasound. During these procedures, two instruments are used via insertion in the rectum for diagnostic measures.
A transrectal ultrasound involves a thin probe used to check the prostate for abnormalities by bouncing high-frequency sound waves off of the wall of internal tissues. The ultrasound device is also used to visualize the prostate and guide a needle into desired zones for tissue extraction.
To examine the prostate cells. a thin needle extracts tissue from the prostate, which is then viewed under a microscope to look for cancer cells. This method identifies cancer and can also indicate how likely that cancer is to spread using the Gleason score.
The main flaw with ultrasound-guided biopsy is that it is random and not aimed at a cancerous or suspicious area on the prostate, since it all typically appears the same on the ultrasound. The urologist cannot be sure if the biopsy of an area will contain cancer cells or not since, overall, approximately 1/100th or less of a gland the size of a peach is being sampled and many cancers may be missed or more aggressive portions of the cancer might not sampled. This could result in missing a prostate cancer diagnosis or underestimating the seriousness of a cancer.
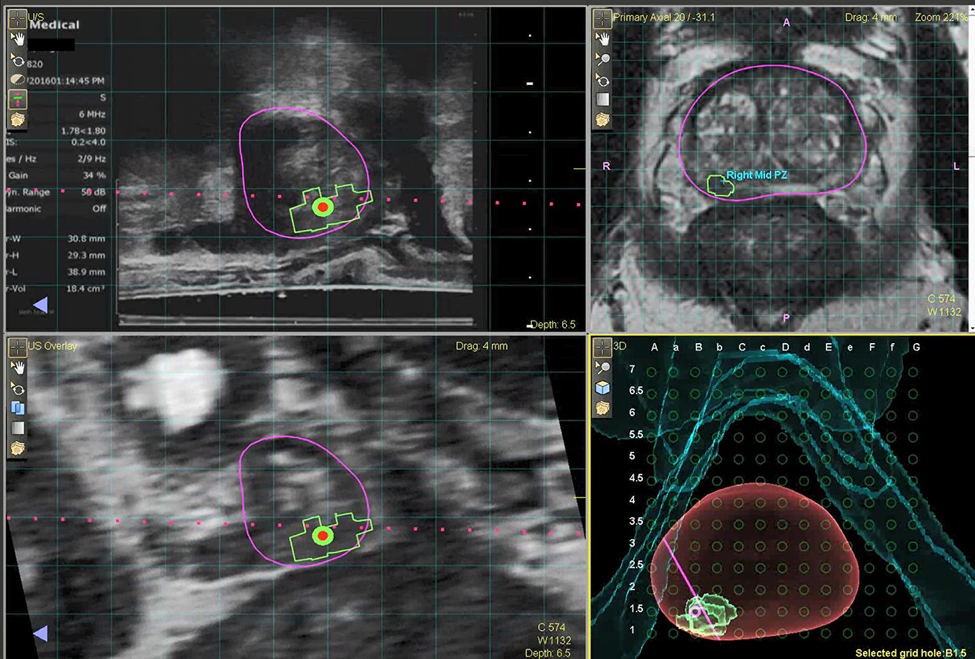
Over the past few years, there has been an increase in the use of Magnetic Resonance Imaging (MRI) to accurately image the prostate with a technique called MRI fusion biopsy.
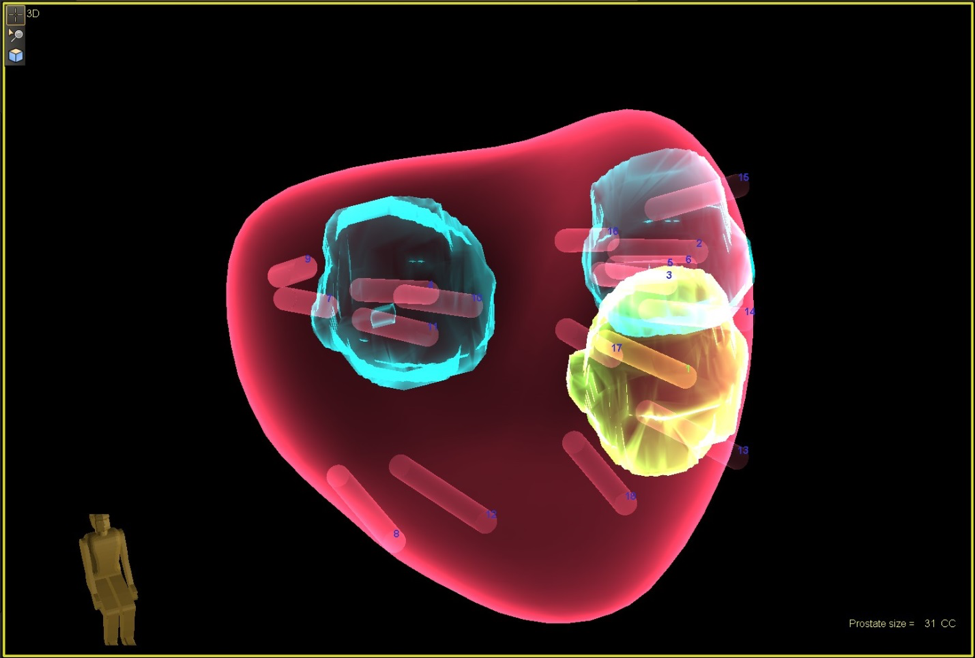
This procedure involves an MRI performed prior to the biopsy to identify lesions in the prostate which may be cancerous, which can then be overlayed on the live ultrasound at the time of biopsy. This enables the urologist to directly target and biopsy any lesions in the prostate in real time and is considered more accurate than a transrectal ultrasound at detecting prostate lesions and obtaining biopsy results.
An accurate biopsy helps to identify which patients are suitable candidates for prostate cancer treatment or for actively watching the cancer (active surveillance).
Treatment
Several factors affect the likelihood of a patient to be cured from prostate cancer, though perhaps the most important is how advanced the cancer has become when treatment begins. When cancer is reserved to a small part of the prostate, it is almost always easier to treat than when it has begun to take over the entire prostate or has spread to other parts of the body. As with most diseases, age and previous levels of health factor into a patient’s likelihood of cure as well.
The aggressiveness of the cancer also plays a major role in the patient’s ability to be cured, as measured by its Gleason score. The Gleason score defines a cancer’s tendency to spread - the lower the number, the slower the cancer should spread.
Current treatments depend on the exact prostate cancer diagnosis and include: active surveillance, radiation, prostate removal (prostatectomy), hormone therapy, High Intensity Focused Ultrasound (HIFU), or chemotherapy. Each patient receives a specialized treatment recommendation based on the pros and cons of each treatment, and the health and age of the patient.
Active Surveillance is a term used to describe closely watching the prostate cancer with scheduled repeat prostate biopsies and monitoring the PSA. This is reserved for patients with low Gleason scores and PSA values. Any increase in the prostate cancer severity may trigger a recommendation of other treatments.
Radiation therapy is a common treatment for cancer of all types. This method involves the use of high levels of energy to kill cancer cells. Although radiation therapy is often an effective treatment, for some patients it can cause side effects such as skin changes, fatigue, swelling, diarrhea, constipation, blood in urine or stool, urge to urinate, and nausea. To treat prostate cancer, two types of radiation treatment are typically used:
External Beam Radiation: This procedure delivers radiation through a powerful beam into the affected area, typically done five days a week for several weeks. This is usually administered with hormone treatments if the Gleason score is higher or the PSA is higher at the time of diagnosis.
Brachytherapy: An alternate form of radiation therapy that involves the placement of tiny radioactive seeds into the affected tissues, delivering a relatively low dose of radiation over a longer period of time. The seeds will eventually cease giving off radiation and do not have to be removed.
Radical Prostatectomy: The full, surgical removal of the prostate which may be performed traditionally, through a full incision in the abdomen, or robotically. Robotic prostatectomy offers doctors the ability to perform surgeries with increased precision and accuracy, as well as decreased blood loss.
Hormone therapy is another treatment used to stave off cancer. Because prostate cancer relies on the male hormone testosterone, cutting that supply off can often lead to cancer cells growing more slowly or even dying off. Methods for reducing or depleting the supply of testosterone vary from medication regimens to full removal of the testicles, the organ that produces testosterone.
High Intensity Focused Ultrasound (HIFU) is a relatively newer technique that treats localized prostate cancer by killing tumor cells with heat. This was approved through the FDA in late 2015. Used alongside MRI fusion biopsy of the prostate, specific locations of prostate which contain cancer can be specifically targeted by HIFU. Targeted cancer treatment is less invasive than surgery for removal of the prostate and typically carries less risk of complications or side effects of surgery or radiation such as sexual side effects and incontinence. For more information, visit Maple Leaf HIFU.
Chemotherapy may be necessary for cases of advanced prostate cancer that are very aggressive or have spread to other organs (metastasize) at the time of diagnosis. If the prostate cancer can no longer be controlled by hormone treatments, it is termed castrate resistant. Our urologists currently offer oral chemotherapy agents for advanced prostate cancer.